Serotonin Syndrome (serotonin toxicity) Serotonergic Syndrome

Serotonin syndrome
Serotonin syndrome also referred to as serotonin toxicity, is a potentially lifethreatening condition associated with increased serotonergic activity in the central nervous system. It is seen with therapeutic medication use, inadvertent interactions between drugs, and intentional selfpoisoning.
Serotonin syndrome may involve a spectrum of clinical findings, which often include mental status changes, autonomic hyperactivity, and neuromuscular abnormalities
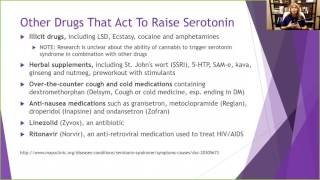
The selective serotonin reuptake inhibitors (SSRIs) are perhaps the most commonly implicated group of medications associated with serotonin syndrome. Notably, SSRIs are less commonly associated with causing severe serotonin syndrome compared with medications that inhibit monoamine oxidase (MAO).
The diagnosis of serotonin syndrome is made solely on clinical grounds. Therefore, a detailed history and thorough physical and neurologic examinations are essential.
Serotonin syndrome encompasses a spectrum of disease where the intensity of clinical findings is thought to reflect the degree of serotonergic activity.
Mental status changes can include anxiety, restlessness, disorientation, and agitated delirium.. Patients may startle easily. Autonomic manifestations can include diaphoresis, tachycardia, hyperthermia, hypertension, vomiting, and diarrhea.
Neuromuscular hyperactivity can manifest as tremor, myoclonus, hyperreflexia, and bilateral Babinski sign. Hyperreflexia and clonus are particularly common; these findings, as well as rigidity, are more often pronounced in the lower extremities.
In severe cases, muscle rigidity may mask myoclonus and hyperreflexia. While uncommon, fatal cases of serotonin syndrome are associated with hyperthermia and seizure, the latter of which is often a preterminal event
Physical examination — Typical vital sign abnormalities include tachycardia and hypertension, but severe cases may develop hyperthermia and dramatic swings in pulse and blood pressure. Dilated pupils, Tremor, Akathisia, Deep tendon hyperreflexia, Inducible or spontaneous muscle clonus, Muscle rigidity & Bilateral Babinski signs.
The differential diagnosis of serotonin syndrome includes neuroleptic malignant syndrome (NMS), anticholinergic toxicity, malignant hyperthermia, intoxication from sympathomimetic agents, sedativehypnotic withdrawal, meningitis, and encephalitis.
Serotonin syndrome is a clinical diagnosis; serum serotonin concentrations do not correlate with clinical findings, and no laboratory test confirms the diagnosis
Five principles are central to the management of serotonin syndrome:
1. Discontinuation of all serotonergic agents
2. Supportive care aimed at normalization of vital signs
3. Sedation with benzodiazepines
4. Administration of serotonin antagonists
5. Assessment of the need to resume use of causative serotonergic agents after resolution of symptoms
Antidote Cyproheptadine is available in 4 mg tablets or 2 mg/5 mL syrup. When administered as an antidote for serotonin syndrome, an initial dose of 12 mg is recommended, followed by 2 mg every two hours until clinical response is seen. Cyproheptadine is only available in an oral form, but it may be crushed and given through a nasogastric or orogastric tube.
Serotonin syndrome is a potentially lifethreatening condition associated with increased serotonergic activity in the central nervous system due to serotonergic agent therapeutic use, inadvertent interactions between drugs, and intentional selfpoisoning




![Delusional Misidentification Syndrome [Capgras Syndrome] Fregoli Syndrome](https://i.ytimg.com/vi/aXZC9c1vYrQ/mqdefault.jpg)