Spirometry Lung Volumes u0026 Capacities Restrictive u0026 Obstructive Diseases Animation.
(USMLE topics, pulmonology) Spirometry explained lung volumes and capacities, changes in restrictive vs obstructive pulmonary diseases. This video and other related videos (in HD) are available for instant download licensing here: https://www.alilamedicalmedia.com//g...
©Alila Medical Media. All rights reserved.
Voice by: Ashley Fleming
Support us on Patreon and get FREE image downloads and video early access: patreon.com/AlilaMedicalMedia
All images/videos by Alila Medical Media are for information purposes ONLY and are NOT intended to replace professional medical advice, diagnosis or treatment. Always seek the advice of a qualified healthcare provider with any questions you may have regarding a medical condition.
Spirometry is a common test for lung function. It is used to diagnose asthma, COPD, pulmonary fibrosis and other lung diseases. It can also be a helpful tool to monitor disease progression, and evaluate effectiveness of a treatment plan. A tubelike device, called a spirometer, is used to capture and record air volumes and breathing speed.
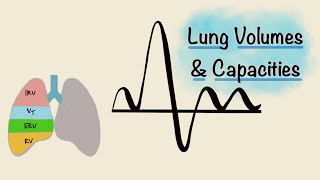
A spirometry test typically reports 4 respiratory volumes:
Tidal volume, TV the amount of air inhaled or exhaled during normal, quiet breathing, without effort.
Inspiratory reserve volume, IRV the amount of air that can be inhaled with maximum effort, after a quiet inhalation.
Expiratory reserve volume, ERV the amount of air that can be exhaled with maximum effort, after a quiet exhalation.
Residual volume, RV – the amount of air remaining in the lungs after a maximum exhalation.
These volumes are used to calculate other parameters, called respiratory capacities:
Inspiratory capacity, IC – the maximum amount of air that can be inhaled after a quiet exhalation.
Functional residual capacity, FRC, the amount of air remaining in the lungs after a quiet exhalation.
Total lung capacity, TLC
And vital capacity, VC – the amount of air that can be exhaled with maximum effort, after a maximum inhalation. This is basically the volume of the deepest breath the lungs can possibly handle, and is an important indicator of pulmonary function, as well as strength of respiratory muscles.
Vital capacity can be measured as slow vital capacity during slow, relaxed breathing; or as forced vital capacity, FVC, when the patient is asked to breathe out as hard and fast as possible. While there is little or no difference between these two values in healthy individuals, people with difficulty exhaling usually show significantly lower FVC.
Another important parameter obtained during forced spirometry is the forced expiratory volume FEV1 the amount of air that is exhaled during the first second of forceful exhalation, after a full inhalation. FEV1 is used to calculate the percentage of air that is expelled during the first second. This FEV1/FVC ratio inversely reflects the resistance to expiratory airflow. In healthy people, it is around 70 to 85%; a smaller number means increased lung resistance.
Spirometry is useful in differentiating between restrictive and obstructive pulmonary diseases. Restrictive lung diseases can be inspiratory or expiratory. Inspiratory restrictive are conditions in which lung compliance is reduced, limiting lung expansion when inhaling. This can happen either because the lungs become “stiff”, as a result of scaring or fibrosis within lung tissues; or the respiratory muscles are too weak to inflate the lungs. Expiratory restrictive is when exhalation volume is limited, due to weakness of accessory muscles involved in deep exhalation. Restrictive lung diseases are associated with decreased lung volumes, or total lung capacity, TLC.
Obstructive lung diseases, such as asthma or COPD, on the other hand, show a normal or somewhat increased total lung capacity, TLC. This is because the obstruction increases lung resistance, making breathing out harder and slower; and this results in increased residual lung volume. Vital capacity remains normal during quiet breathing, but when breathing rapidly, a higher pressure is required to overcome the increased resistance, and forced vital capacity is reduced. A more reliable indicator of obstructive lung disease, however, is the lower percentage of air that is exhaled during the first second of forceful exhalation.