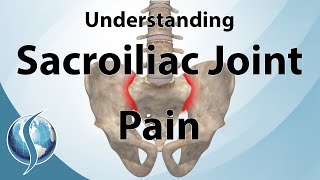
sacroiliac Joint pain why it Hurts - Everything You Need To Know - Dr. Nabil Ebraheim
Dr. Ebraheim’s educational animated video describes information about the sacroiliac joint (SI joint) and why does it hurt?.
Follow me on twitter:
https://twitter.com/#!/DrEbraheim_UTMC
Find me on Instagram @OrthoInitiative
The Si joint is frequently overlooked as an important cause of low back pain in about 22% of the cases. It is present in about 40% of all ow back pain patients that had spinal fusion.
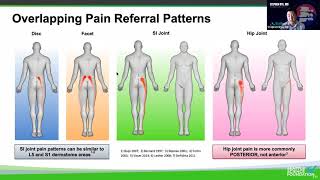
What is the SI joint? This is the spine. This is the sacrum which is the lower part of the spine. The pelvis is connected to the spine through the SI joints. Why is this connection important? Because the SI joint transfers the force and the load from the spine to the legs. The Si joint has very little movement; you don’t want a lot of movement. The Si joint is limited to less than four degrees pf rotation and bout 1.6 mm of translation, so the SI joint has very little movement. The cause of the pain in the SI joint cannot be due to this little movement. Some people think it is neuroplasticity when the nervous system is very sensitive to any movement and the ligaments around the SI joint is full of nerve fibers. Neuroplasticity is rewiring of the nervous system in response to injury to function differently than before. It is a maladaptive reorganization of the nervous system to a painful site which can be resolved with treatment. In general, the cause of the pain is usually difficult to determine. SI joint is protected by strong ligaments that prevent shear forces, and it is surrounded by strong muscles for stabilization during movement. The causes of SI joint problems are several. Pain from different sources overlap. The SI joint, the lumbar spine, and the hip share the same pain. The pain may be associated with one of these areas or all of these areas. In fact, more than one source of pain may exist. So the diagnosis of SI joint dysfunction can be challenging and the patient will go through a battery of steps including injection with greater than 75% in reduction of pain. The cause of the pain is usually idiopathic and multiple risk factors may exit. Usually, the idiopathic SI joint dysfunction will not show up on the xray, MRI, or CT. In fact, up to 25% of asymptomatic patients over 50 years old will have abnormal SI joints on xrays.Risk factors / causes of SI joint pain? The important risk factor is previous lumbar fusion, especially when there is more than three levels involved, similar to adjacent segment disease. So if the spine is fused, then maybe the SI joint will move more and become painful. Pregnancy can cause SI joint pain. Previous trauma to the pelvis can cause SI joint pain. 80% of patients have a history of a specific trauma, usually a twisting injury. And Si joint pain can occur from getting bone graft from the pelvis and violating the SI joint. Always obtain a detailed history of trauma, infection, inflammatory disease such as Ankylosing Spondylitis, Reiter’s Syndrome, Psoriasis, check for spinal fusion, Scoliosis and leg length discrepancy. When you examine the patient, the pain is usually not in the midline, the pain is usually to the side. The pain will be below L5 level. How do you now that? Look at that pelvis. This is the level of the iliac crest and this line corresponds to the L4 level. The pain will be below the L5 level. Only 4% of patients had pain above L5. Usually, the SI joint pain is just inferior to the posterior superior iliac spine (PSIS). Treatment of the SI joint is usually nonoperative treatment including antiinflammatory medication, physical therapy and pelvic belt. Try to do at least four weeks of nonoperative treatment before doing the injection. If you suspect the SI joint to be the cause or the main pain generator, then you need to identify the area of pain exactly, and that will be done by a diagnostic injection to confirm the diagnosis. The injection might give 60% success rate in pain relief at six months. If you have more than 75% reduction of the SI joint following a single injection, that means that the source of pain is the SI joint. You have to do it under fluoroscopy or ultrasound. If you do it blind, only 22% of the needles will be in the SI joint. Injection can be diagnostic and therapeutic, but do not give more than three injections in six months or four injections within one year. The radiofrequency ablation targets the lateral branches of the sacral nerve roots, but it is unable to denervate the anterior neural structures of the Si joint. Fusion is minimally invasive. You have got to have confirmation that the pain comes from the SI joint, the SI joint is the primary pain generator, and you have to have poor response from nonoperative treatment. The procedure can be done minimally invasive and as an outpatient. Result has better outcome compared to conservative treatment. Arthrodesis is good option for a patient with confirmed sacroiliac joint dysfunction and poo response to nonoperative treatment. SI dysfunction is a disabling problem.



![Your Piriformis Isn't Tight, it's WEAK! [4 Exercises to Get it Strong]](https://i.ytimg.com/vi/yBRSQB0Xyb0/mqdefault.jpg)


![Your Psoas Isn't Just Tight, It's WEAK [Don't Stretch, Do These Instead]](https://i.ytimg.com/vi/h_srhkcJxAY/mqdefault.jpg)